USMLE GIT 8: Hernias Made Easy! (Plus Diverticulums)
Автор: LY Med
Загружено: 2017-06-15
Просмотров: 12806
Want to support the channel? Be a patron at:
/ lymed Welcome to LY Med, where I go over everything you need to know for the USMLE STEP 1, with new videos every day.
Follow along with First Aid, or with my notes which can be found here: https://www.dropbox.com/sh/m55dzy5jju...
This video is all about hernias and diverticulums. We'll start with hernias. Just some terminology:
A reducible hernia is when you can press it back in.
An incarcerated hernia cannot be reduced
If it starts to lose it's blood supply, it's a strangulated hernia
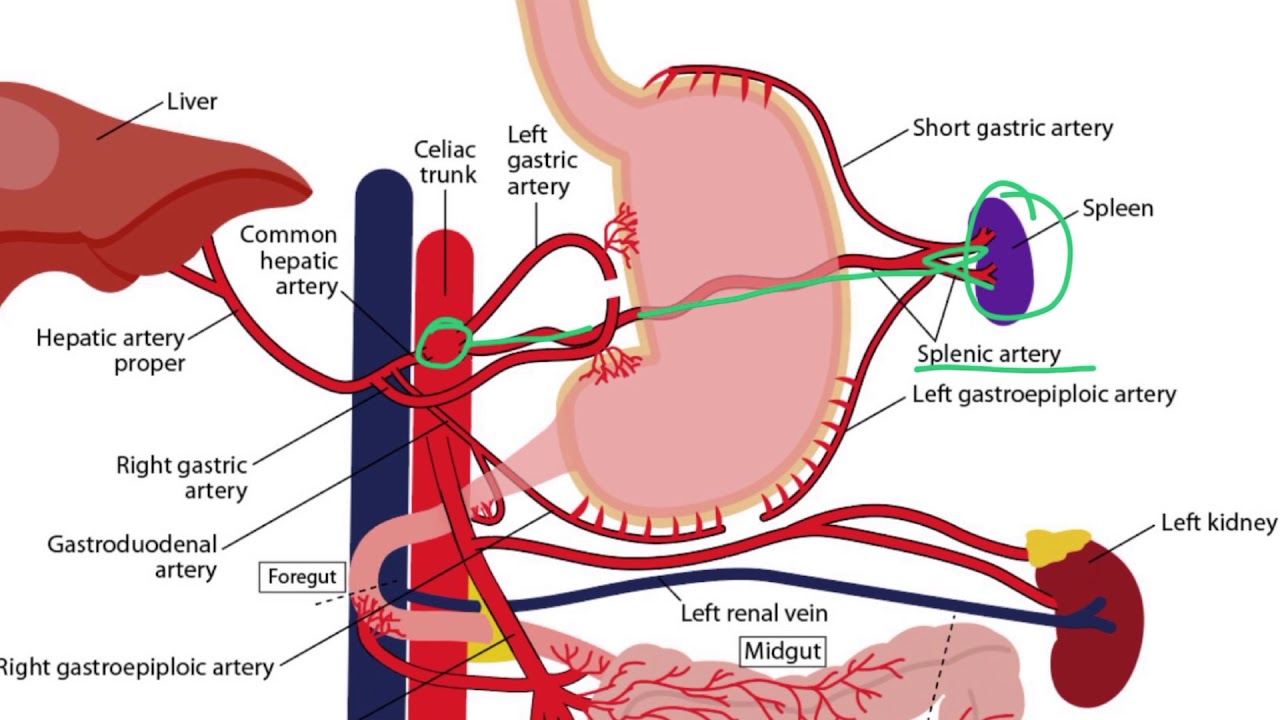
Now where can your GIT herniate through? One area is the diaphragm. Some other areas include the femoral area (femoral hernia) and the inguinal canal (inguinal hernia). Let's talk about diaphagmatic hernias first. You can either have sliding hiatal hernias, in which your cardia of the stomach moves up, or you can have paraesophageal hernias. These predipose patients to GERD. Some patients are born with these hernias and can affect lung development, leading to respiratory distress at birth and bowel sounds on auscultation of the lung.
Now let's move onto femoral hernias. These sit below your inguinal ligament and affects women more due to their larger pelvis. Other structures in this area include femoral nerves, femoral veins, and lymphatics.
Last but not least, we have inguinal hernias. To understand inguinal hernias, you need to understand the inguinal canal. You have a superficial opening called the external ring, which is draped by the external spermatic fascia. More internally, you have the deep internal ring (internal opening). Lastly, there is an artery that bisects the canal called the inferior epigastric artery. So now that you know that anatomy, you can understand the pathology of inguinal canals. You can herniation right through the external openinng. We call these DIRECT inguinal hernias, and these are medial to the inferior epigastric artery. The second type goes through the internal ring and we call this indirect hernias. This travels through the canal and into the testes. That does it for hernias!
Now let's move onto another topic- diverticulums. This is so common it's probably just normal physiology. These are outpouching of your GIT, especially where the vasa recta perforate. Often it's seen in the sigmoid colon and associated with constipation. This can progress to diverticulosis and rectal bleeding, or hematochezia. These outpouching can get infected and turn into diverticuLITIS. This can perforate your bowels and create fistulas.
Now you can have outpouchings in other parts of your GIT. For example, you can have an outpouching in your esophagus. We call this Zenker's diverticulum. This can be due to increased pressure from dysphagia and leads to halitosis. You can also have something called a Meckel's diverticulum. This is due to the failure of the vitelline duct to involute. If it nevers involutes, you can have this outpouching. Something important to know, Meckel's diverticulum also contains gastric and pancreatic tissue. We can test for these tissue with technetium scans.
Done!
Доступные форматы для скачивания:
Скачать видео mp4
-
Информация по загрузке: